‘Strange things’ in egg breakout – when to suspect a breeder nutrition problem
Tags: Incubation | Whitepaper
, 3 November 2025

If the hatchability is lower than expected, a very useful tool to help pinpoint the direction in which to look is an egg breakout of both candled and unhatched eggs.
Normal expectations of embryonic mortality
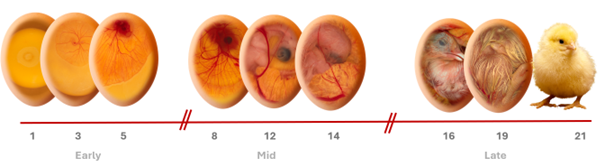
In practice, roughly three sub-groups are recognised during a breakout: early, mid and late embryonic death. The probability of embryonic death is highest in early and late embryonic development.

When to suspect a problem in the breeder flock
When encountering high embryonic mortality, many variables need to be evaluated. These include failure in egg turning, very high or low temperatures, and egg handling mistakes (including storage conditions and disinfection). Once incubation and egg handling related mistakes have been excluded, attention usually turns to the breeder flock. Genetics, disease, stress, drugs, the coccidiostat Nicarbazin, toxins, parasitic infection and vitamin and mineral deficiencies can all result in higher embryonic mortality. Here we focus on vitamin and mineral deficiencies. The more severe the shortage or overdosing, the stronger and earlier the effect will appear during embryonic development.
Possible nutrition-related signs during breakout
Week 1 (early) – Abnormalities become more obvious during the later stages of embryonic development, when it is easier to recognise skeleton deformities, haemorrhages, edema, poor feathering, and so on. For early mortality, the ‘signs’ are less clear – other than simply a higher number of more or less normal looking embryos that died in the early stages of development. Pay special attention at around days 2 and 3 (the ‘membrane’ and ‘blood ring’ stages, respectively), as vitamin A and E deficiencies are known to negatively influence vascular development. A high level of early embryonic mortality can indicate a deficiency in vitamin A, riboflavin, biotin, vitamin E, thiamine, selenium or copper. During an egg breakout, early embryonic deaths in the first 48 hours of incubation (‘membrane stage’) should not be mistaken for infertile eggs.
Week 2 (mid) – Mid mortality is normally lower than 1%. If embryonic death is higher than 1% and you see skeleton deformities, edema or haemorrhages during egg breakout, it is wise to check potential deficiencies in riboflavin or pantothenic acid. High mid-embryonic mortality is almost never related to incubation problems.
Week 3 (late) – Depending on the severity of the deficiency, the embryo dies in an earlier or later stage of development. Some vitamin or mineral deficiencies (vitamin D3, biotin, folic acid, thiamine, zinc, manganese) can cause skeleton deformities (e.g. dwarfism or beak deformities), which complicate the hatching process, causing the embryo to die before or during the hatching process. Other signs can be clubbed down (riboflavin), curled toes (riboflavin, vitamin B12), soft bones/rubbery beak (vitamin D3), encephalomalacia (vitamin E) or edema (riboflavin, vitamin B12, manganese).
Advice
- Consider breeder nutrition if embryo mortality rates are higher than standard, especially in more than one breeder flock receiving feed from same supplier.
- Be alert to malformations in embryos; these might point to an issue with breeder nutrition.
- Breeder farms should keep feed samples from each feed delivery to be used for reference and analysis.
- Be aware that after a nutritional problem is detected, it can take a few weeks before hatch results increase again.
References available on request
Written by Lotte Hebbink
Incubation specialist
I welcome your feedback on this article - and if you require any additional information, please don't hesitate to contact me.